Pe măsură ce metaboliții intestinali mirositori traversează bariera peretelui intestinal și ficatul, aceștia sunt excretați prin transpirație și respirație. Simptomele rezultate se numesc bromhidroză și halitoză.
Limbi: BG | ZH | ZH-CN | ZH-HK | ZH-TW | CS | CS-CZ | DA-DK | NL | NL-BE | NL-NL | EN | EN-AU | EN-AT | EN-BE | EN-CA | EN-CN | EN-EN | EN-EG | EN-DE | EN-IN | EN-IE | EN-MY | EN-NZ | EN-NG | EN-PH | EN-ZA | EN-GB | EN-US | ET-EE | FI | FI-FI | FR | FR-BE | FR-CA | FR-FR | FR-CH | DE | DE-AT | DE-DE | DE-CH | EL | EL-GR | HU | HU-HU | IT | IT-IT | IT-CH | JA | JA-JP | KO-KR | NB | PL | PL-PL | PT | PT-BR | PT-PT | RO-RO | RU | RU-RU | SK | SK-SK | SL-SI | ES | ES-AR | ES-CO | ES-LA | ES-MX | ES-PE | ES-ES | ES-US | ES-VE | ES-XL | SV | SV-SE | TR | TR-TR | UK-UA |
Cum să vă înscrieți?
Pacienții cu IMBS se pot înscrie într-un registru internațional de pacienți care este găzduit la CoRDS (Sanford Research) platformă.
Informații mai detaliate despre registrul pacienților se găsesc în următorul pliant: Pliant de informare privind registrul pacienților
Recomandăm fiecărui pacient să se înscrie în registru, deoarece setul de date din acest registru de pacienți reprezintă o bază pe care cercetătorii se bazează pentru a lua decizii fundamentale cu privire la o investigație și la ce fel de investigații într-o cohortă de pacienți cu boli rare.
Notă:
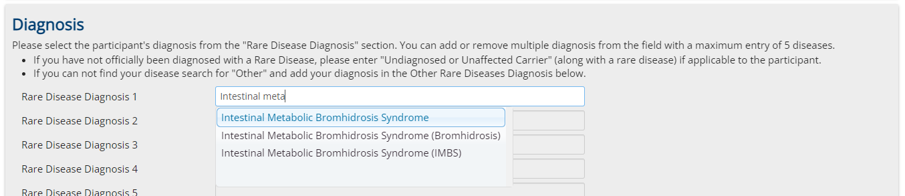
Este foarte important să alegeți în prima pagină de înregistrare "Sindromul de bromhidroză metabolică intestinală" ca boală rară. (Alegeți acest lucru și în cazul în care este doar suspectată și nu este încă diagnosticată)
Raport:
Puteți descărca un raport actualizat automat, bazat pe un subset de date din registru, de la următorul link:
Nu ne lăsați să ne facem treaba singuri! Nu fiți pasivi - acționați! Acționați împreună cu noi!
Suntem oameni ca tine, care lucrăm pe toate fronturile pentru ca această boală să fie recunoscută, stabilită în medicină și rezolvată!
Alătură-ți forțele alături de noi, susține-ne cu tot ceea ce ne poți susține!
Spuneți tuturor celor la care vă gândiți, despre acest text, despre acest grup și despre obiectivele noastre! Spune-le să se alăture!
Nimeni nu primește bani pentru asta, dar poate că ne vom recupera cu toții viețile, viața socială, viața profesională, totul!
Împărtășește peste tot link-uri către comunitatea noastră, adu oamenii împreună - alătură-te alianței noastre, fii membru alături de noi!
Nu ezitați, nu fugiți singuri, susțineți-ne și fiți susținuți de noi!
Nu fiți pasivi - acționați!
