Коли пахучі кишкові метаболіти проникають через бар'єр кишкової стінки та печінку, вони виводяться з потом та диханням. Симптоми, що виникають в результаті, називаються бромгідрозом та галітозом.
Мови: BG | ZH | ZH-CN | ZH-HK | ZH-TW | CS | CS-CZ | DA-DK | NL | NL-BE | NL-NL | EN | EN-AU | EN-AT | EN-BE | EN-CA | EN-CN | EN-EN | EN-EG | EN-DE | EN-IN | EN-IE | EN-MY | EN-NZ | EN-NG | EN-PH | EN-ZA | EN-GB | EN-US | ET-EE | FI | FI-FI | FR | FR-BE | FR-CA | FR-FR | FR-CH | DE | DE-AT | DE-DE | DE-CH | EL | EL-GR | HU | HU-HU | IT | IT-IT | IT-CH | JA | JA-JP | KO-KR | NB | PL | PL-PL | PT | PT-BR | PT-PT | RO-RO | RU | RU-RU | SK | SK-SK | SL-SI | ES | ES-AR | ES-CO | ES-LA | ES-MX | ES-PE | ES-ES | ES-US | ES-VE | ES-XL | SV | SV-SE | TR | TR-TR | UK-UA |
Як зареєструватися?
Пацієнти ММБС можуть зареєструватися в міжнародному реєстрі пацієнтів, який розміщений на сайті CoRDS (Sanford Research) платформу.
Більш детальну інформацію про реєстр пацієнтів можна знайти у наступному флаєрі: Інформаційна листівка про реєстр пацієнтів
Ми наполегливо рекомендуємо кожному пацієнту зареєструватися в реєстрі, оскільки набір даних цього реєстру пацієнтів є базою, на яку спираються дослідники, приймаючи принципові рішення про проведення дослідження і про те, які саме дослідження проводити в когорті пацієнтів з рідкісним захворюванням.
Зауважте:
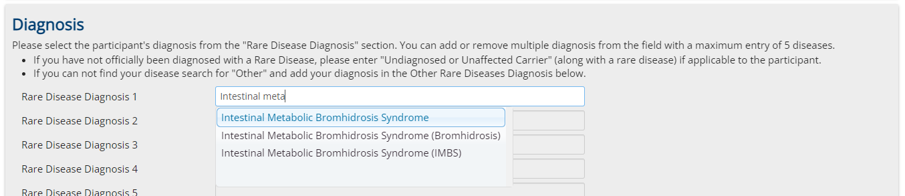
Дуже важливо на першій сторінці реєстрації обрати "Синдром кишкового метаболічного бромгідрозу" як рідкісне захворювання. (Також обирайте це у випадку, якщо це захворювання лише підозрюється, але ще не діагностоване)
Доповідайте:
Завантажити автоматично оновлений звіт на основі підмножини даних реєстру можна за наступним посиланням:
Не дайте нам зробити роботу самотужки! Не будьте пасивними - дійте! Дійте разом з нами!
Ми - такі ж люди, як і ви, працюємо на всіх фронтах, щоб цю хворобу визнали, закріпили в медицині та подолали!
Об'єднуйте зусилля з нами, підтримуйте нас усім, чим можете підтримати!
Розкажіть про цей текст, про цю групу і про наші цілі всім, про кого зможете згадати! Закликайте приєднуватися!
Грошей за це ніхто не отримає, але, можливо, нам усім повернуть наше життя, наше соціальне життя, наше робоче життя, все!
Поширюйте скрізь посилання на нашу спільноту, об'єднуйте людей - приєднуйтесь до нашого альянсу, будьте учасником пліч-о-пліч з нами!
Не зволікайте, не біжіть поодинці, підтримуйте нас і будьте підтримані нами!
Не будьте пасивними - дійте!
