As odorous intestinal metabolites cross the intestinal wall barrier and liver they are excreted in sweat and breath. The resulting symptoms are called Bromhidrosis and Halitosis.
Languages: BG | ZH | ZH-CN | ZH-HK | ZH-TW | CS | CS-CZ | DA-DK | NL | NL-BE | NL-NL | EN | EN-AU | EN-BE | EN-CA | EN-CN | EN-EN | EN-DE | EN-IE | EN-MY | EN-NZ | EN-NG | EN-PH | EN-ZA | EN-GB | EN-US | ET-EE | FI | FI-FI | FR | FR-BE | FR-CA | FR-FR | FR-CH | DE | DE-AT | DE-DE | DE-CH | EL | EL-GR | HU | HU-HU | IT | IT-IT | IT-CH | JA | JA-JP | KO-KR | NB | PL | PL-PL | PT | PT-BR | PT-PT | RO-RO | RU | RU-RU | SK | SK-SK | SL-SI | ES | ES-AR | ES-CO | ES-LA | ES-MX | ES-PE | ES-ES | ES-US | ES-VE | ES-XL | SV | SV-SE | TR | TR-TR | UK-UA |
How to enroll?
IMBS patients can enroll themselves in an international patient registry that is hosted at the CoRDS (Sanford Research) platform.
Please find more detailed information about the patient registry in the following flyer: Patient Registry Info Flyer
We highly recommend each and every patient to enroll in the registry as the data set of this patient registry is a base which researchers rely on to make fundamental decisions about an investigation and which kind of investigations in a rare disease patient cohort.
Note:
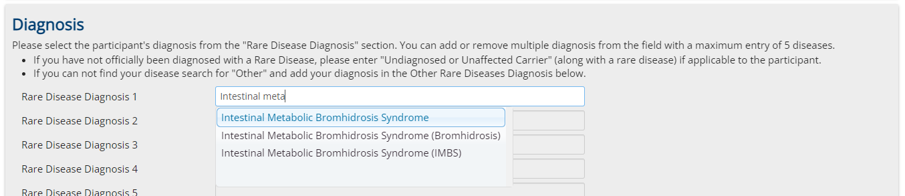
It is very important to choose in the first registration page "Intestinal Metabolic Bromhidrosis Syndrome" as rare disease condition. (Also choose this in the case it is only suspected and not diagnosed yet)
Report:
You can download an automatically updated report based on a subset of the registry data from the following link:
Don't let us do the job alone! Don't be passive - act! Act together with us!
We are people like you, working on every front to get this disease recognized, established in medicine and solved!
Join forces with us, support us with everything you can support us with!
Tell everyone you can think of, about this text, about this group and about our goals! Tell them to join!
No one gets money for this, but maybe we all get our lives back, our social life, our work life, everything!
Share links everywhere to our community, bring the people together - join our alliance, be a member side by side with us!
Don't hesitate, don't run alone, back us up and get backed up by us!
Don't be passive - act!
